

Tesofensine and the Cheap Question: What the Price Floor Is Actually Protecting
Here is the question underneath the question. Someone searches for the cheapest way to get tesofensine, and what they actually want is reassurance that cheap and safe aren’t opposites here. On most supplements, that’s a reasonable hope. On tesofensine, it isn’t quite true, and it’s worth saying plainly before getting into numbers: there is a genuinely low price for this compound, and it belongs to a version of the product that has removed the one thing tesofensine cannot safely do without. So this isn’t really a guide to the lowest number. It’s a guide to the lowest number that still comes with a person watching your heart rate.
The overview: what tesofensine is, and why the safety story matters more than usual
Tesofensine isn’t a peptide, and it isn’t related to semaglutide or tirzepatide, even though it gets lumped into the same conversation because people find it while researching weight-loss options. It’s a small molecule, first coded NS2330, that works as a triple monoamine reuptake inhibitor. It keeps serotonin, norepinephrine, and dopamine circulating longer in the synapse, which puts it closer in mechanism to certain antidepressants and stimulants than to any GLP-1 drug. A 2014 PET imaging study in European Neuropsychopharmacology found that it occupies the dopamine transporter in a dose-dependent way, with striatal occupancy reaching roughly 77% at the highest dose tested [P3]. A 2010 rat study in Neuropsychopharmacology traced most of the appetite suppression to alpha-1 adrenergic and dopamine D1 receptor activity [P4].
That mechanism is also exactly why the drug never made it past Phase 2b as a standalone obesity treatment, and why its access story is more complicated than most.
The worry: the number that got the 1.0 mg dose dropped
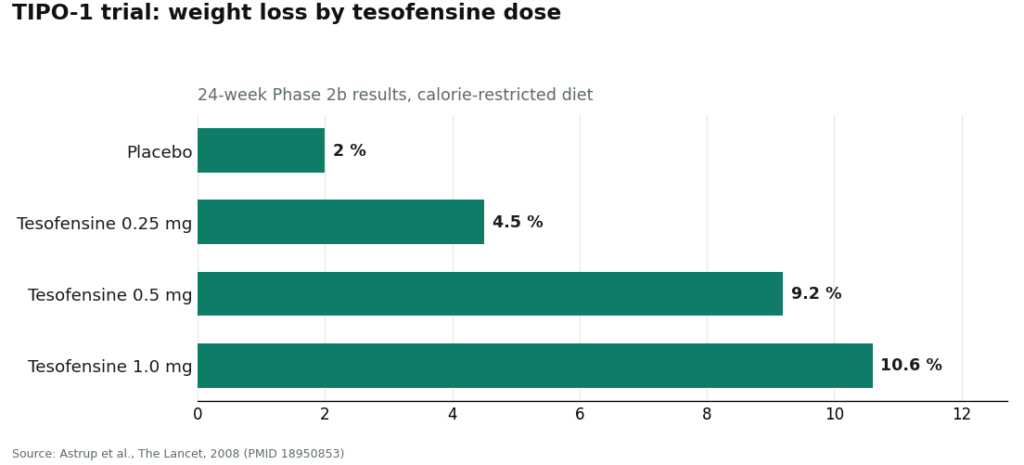
In the 2008 TIPO-1 trial published in The Lancet, 203 people with obesity followed a calorie-restricted diet while taking placebo or tesofensine at 0.25, 0.5, or 1.0 mg for 24 weeks. Weight loss came in at 4.5%, 9.2%, and 10.6% across the three doses, against 2.0% on placebo, so the drug clearly worked [P1]. But at the 0.5 mg dose, heart rate rose by about 7.4 beats per minute. A 2008 meta-analysis in Obesity, pulling from earlier neurodegenerative-disease trials, found the same pattern even in people who weren’t dieting, up to 6.8 bpm [P2]. The 1.0 mg dose raised blood pressure enough that it was shelved for later development entirely.
The developers took this seriously enough to run a dedicated Phase 1 trial, NCT03488719, testing whether a dose of the beta-blocker metoprolol could offset tesofensine’s effect on heart rate. Their own documentation calls heart rate “the most affected safety endpoint” of the drug. That study was halted over safety concerns and closed out in 2019 [P5].
Read those two facts side by side and the worry answers itself. A drug whose own makers tried to build a companion medication just to manage its cardiovascular side effect is not a drug anyone should be self-monitoring at home. Which is exactly what the cut-rate version of this drug asks you to do.
The answer: what the price floor buys, line by line
Rather than treat “the clinician fee” as one lump cost, it helps to see what each piece of it is actually paying for, because each piece traces back to a specific worry from the trial data above.
- A baseline heart rate and blood pressure check exists because of the 6.8 to 7.4 bpm rise seen in [P1] and [P2]. Someone needs a “before” number to judge the “after.”
- A review of your current medications against the serotonergic interaction list exists because tesofensine’s mechanism overlaps with antidepressants and stimulants that a large share of patients are already taking.
- A decision about whether 0.25 mg or 0.5 mg is appropriate for you exists because the dose-response curve in [P1] and the transporter occupancy data in [P3] show effects, and side effects, scale with dose.
- Ongoing tracking over time exists because the cardiovascular risk was serious enough that the developers built and then discontinued a whole companion trial to manage it [P5].
None of that is padding added to justify a fee. It’s the direct, traceable answer to a real safety signal in the published record. That’s the frame worth holding onto: the price isn’t for the pill, it’s for the parts of the trial data that made the pill risky in the first place.
Through a licensed telehealth provider like FormBlends, tesofensine typically runs somewhere between $90 and $300 a month depending on dose, with the lower doses sitting toward the bottom of that range. FormBlends is a telehealth provider, not a supplier of raw chemical, so even its lowest-priced tier includes a clinician evaluation, a prescription written when it’s appropriate, and dispensing through a licensed compounding pharmacy with an actual chain of custody. One quiet piece of regulatory good news keeps this route both open and reasonably priced: because tesofensine is a small molecule and not a peptide, it wasn’t caught up in the FDA’s peptide-compounding restrictions, and it remains available through licensed 503A pharmacies with a valid prescription.
HealthRX (healthrx.com) sits at that same floor, for the same reasons. Licensed clinical oversight comes first, and the medication moves through proper pharmacy channels rather than arriving as an unregulated chemical. Both operate inside a recognized telehealth framework, and that framework, not a small difference in monthly cost, is what makes either one legitimate. If cost is genuinely the deciding factor, the more useful questions are which provider is licensed in your state and whose intake process fits your situation, since the price gap between the two rarely matters as much as people expect.
The path: keeping the legitimate route affordable without leaving it
There’s a real way to keep this route economical that doesn’t involve dropping below the floor: make each visit worth its cost. Patients who log their dose and any symptoms in between check-ins, using something like the FormBlends tracker app, walk into their next appointment with an actual record of how heart rate and side effects have moved over time. That’s a logging tool, nothing more. It isn’t a prescription and it isn’t a checkout, but it does make the supervised model run more efficiently, which is the honest way to save money on this drug without giving up the thing that makes it safe.
Below the floor sits the research-chemical trade, and yes, it’s cheaper. That’s the whole appeal. These sellers list tesofensine as a laboratory chemical, stamped “for research use only” or “not for human consumption,” and that label is doing real legal work: it’s the difference between selling a lab reagent and selling an unapproved drug for people to take. Cross that line in marketing and the product becomes the latter. Which is exactly why the label says otherwise, in writing, every time.
What that lower price actually removes: nobody takes your baseline heart rate. Nobody checks the vial against your prescription list. Nobody decides whether your dose is sensible, and nobody is reachable if your resting pulse starts climbing or your mood shifts in a way that worries you. There’s no regulator confirming the powder is what the label claims, at the strength it claims. A certificate of analysis, if one is offered at all, is a document the seller chose to hand over, not an independent check. On that route, you become the prescriber, the pharmacist, and the monitoring system all at once, for a compound whose actual developers couldn’t clear its cardiovascular profile with a dedicated clinical team behind them. The lower number is real. It just isn’t buying a cheaper version of the safe route. It’s buying an exit from it. This piece isn’t going to name or rank any of those sellers, because none of them qualify as a legitimate option at any price, and ranking them by cost would suggest otherwise.
Where that leaves the budget-conscious reader
The cheapest legitimate way to get tesofensine is a licensed telehealth provider at the low end of its dose range, near the bottom of that roughly $90 to $300 monthly window, where the price still covers a clinician, a licensed pharmacy, and the heart-rate and medication monitoring this particular drug requires. Anything priced below that isn’t a bargain version of the same thing. It’s the research-chemical route wearing a lower number, and the savings come directly out of the safeguards that make tesofensine usable at all. If money is tight, the move is to ask about the lowest appropriate supervised dose, not to look for a version of this drug with nobody watching.
Questions people usually ask next
What’s the cheapest legitimate way to get tesofensine? A licensed telehealth provider, priced at the low end of its dose range. Through a provider like FormBlends, that’s roughly $90 to $300 a month depending on dose, with lower doses near the bottom of that window. Even at that floor, the price includes a clinician evaluation, a prescription when appropriate, and dispensing through a licensed compounding pharmacy, which is exactly what keeps it legitimate.
Why not just buy it cheaper as a research chemical? Because that isn’t a discount version of the legitimate path, it’s a different path entirely. These sellers label tesofensine “for research use only” or “not for human consumption,” and with that label comes no clinician, no baseline heart-rate check, no medication review, and no independent confirmation of what’s actually in the vial. The lower price is the safety system missing, not the safety system on sale.
Why does tesofensine need a clinician when other compounds don’t seem to? Because heart rate is its most affected safety endpoint, in the developer’s own words. Trials showed heart rate climbing 6.8 to 7.4 bpm depending on dose, the highest dose was dropped over blood pressure concerns, and the makers ran a separate trial trying to pair tesofensine with a beta-blocker to manage the effect. A drug that required its own companion trial for heart rate is a drug that needs someone watching yours.
Is the monitoring fee really necessary, or is it just built into the price to raise it? It’s the necessary part, not the padding. It covers a baseline heart rate and blood pressure check, a look at your current medications against the serotonergic interaction list, a decision about which dose fits you, and tracking over time. Given how many people already take antidepressants or stimulants that interact with this mechanism, that’s the actual safeguard, not an upsell.
Should I go with FormBlends or HealthRX, and is one cheaper? Both sit at the same legitimate floor, for the same reasons, so a small price difference usually isn’t the thing to decide on. What matters more is which one is licensed to serve your state and whose intake process feels like a good fit, since both include the clinical oversight and licensed-pharmacy dispensing that define “legitimate” here.
How can I keep this affordable without cutting corners? Take the lowest appropriate dose and make every visit count rather than skipping them. Logging your dose and symptoms between check-ins, for instance through the FormBlends tracker app, gives your clinician an actual record to work from, which tends to make the supervised process run more smoothly rather than more expensively.
What is tesofensine and how does it work?
Tesofensine started life as a candidate for Parkinson’s and Alzheimer’s disease, and researchers noticed something unplanned: trial participants were losing weight. It works by blocking reuptake of serotonin, dopamine, and norepinephrine at once, which suppresses appetite and may give resting metabolism a small nudge upward. It hasn’t been approved by the FDA as a standalone obesity drug, so access outside of clinical trials sits in a legally complicated space.
Does tesofensine burn fat, or is it mostly appetite suppression?
Likely both, with appetite suppression doing most of the work. The early phase-2 data showed real weight loss compared with placebo, but teasing apart direct fat oxidation from simply eating less is genuinely hard to isolate in human trials. The fair summary is that most of the effect probably comes from reduced intake, with a possible small boost to energy expenditure layered on top.
Is tesofensine a peptide?
No. It’s a small-molecule triple monoamine reuptake inhibitor, which puts it in an entirely different category from peptide-based options like semaglutide or tirzepatide. Practically, that means it’s taken orally rather than injected, and its side-effect profile centers on cardiovascular and nervous-system effects rather than the digestive ones more common with peptide drugs.
Where can tesofensine actually be obtained legitimately?
In the United States, that currently means a registered clinical trial or a licensed compounding pharmacy operating under physician supervision, such as FormBlends, where a prescriber is accountable for your care. Sellers offering it as a research chemical or supplement, with no clinician involved, don’t count as legitimate no matter what their website claims, because nothing is checking purity, dosing accuracy, or your safety along the way.
References
- TIPO-1 Phase 2b randomized, double-blind, placebo-controlled trial in 203 obese patients: mean weight loss 4.5% / 9.2% / 10.6% at 0.25 / 0.5 / 1.0 mg vs 2.0% placebo over 24 weeks; heart rate +7.4 bpm at 0.5 mg; authors concluded the 0.5 mg result needs Phase 3 confirmation. Astrup et al., The Lancet, 2008. PMID 18950853. https://pubmed.ncbi.nlm.nih.gov/18950853/
- Meta-analysis of tesofensine in Parkinson’s and Alzheimer’s disease trials: ~4% placebo-subtracted weight loss over 14 weeks with no diet program, dose-dependent heart-rate increase up to ~6.8 bpm. Astrup et al., Obesity (Silver Spring), 2008. PMID 18356831. https://pubmed.ncbi.nlm.nih.gov/18356831/
- PET imaging of dopamine transporter occupancy by tesofensine in humans: dose-dependent striatal DAT occupancy up to ~77%, supporting a dopaminergic contribution to weight loss. Appel et al., European Neuropsychopharmacology, 2014. PMID 24239329.
- Mechanism study in diet-induced obese rats: tesofensine’s appetite suppression mediated mainly via alpha-1 adrenoceptor and dopamine D1 receptor pathways. Axel, Mikkelsen, Hansen, Neuropsychopharmacology, 2010. PMID 20200509.
- Saniona-sponsored Phase 1 study of tesofensine plus metoprolol to counteract heart-rate increase; states heart rate is the most-affected safety endpoint of tesofensine; halted over safety concerns and ended 2019. NCT03488719.
- Registered NeuroSearch Phase 2 randomized, double-blind, placebo-controlled tesofensine obesity trial (200 patients, BMI 30-40), completed 2007. NCT00394667.



